
Primary Health Care for Universal Health Coverage.


Health Is Your Right & Responsibility
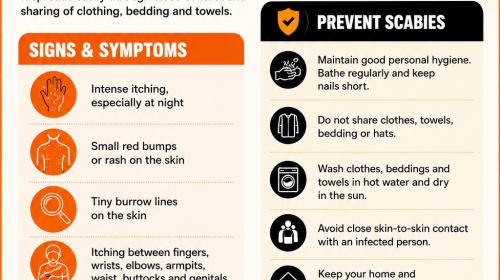
Scabies is a contagious skin condition that spreads through close skin-to-skin contact and the sharing of clothing, bedding, or towels. Early recognition of symptoms and prompt medical attention are key to preventing further transmission.
The CWGH encourages everyone to practise good personal hygiene, avoid sharing personal items, wash clothing and bedding regularly, and seek care at the nearest health facility if symptoms develop.
Together, we can reduce the spread of scabies and protect the health of our communities.
Health is built not only in hospitals – but also in national budgets.
As SADC Ministers of Finance & Health meet in Harare, the focus is on sustainable health financing to ensure quality healthcare for all.
CWGH is proud to be part of this important conversation through Executive Director, Itai Rusike (extreme right).  CWGH is participating in these important regional discussions to advocate for equitable, people-centred and accountable health financing that leaves no one behind.
CWGH is participating in these important regional discussions to advocate for equitable, people-centred and accountable health financing that leaves no one behind.
We are proud to unveil the CWGH Annual Report for 2025 — a compelling testament to our unwavering commitment to advancing health, health rights, and social justice in Zimbabwe.
Follow Link for details: https://drive.google.com/file/d/1zs4ONsrwX-DPrkE0R4s-Cnucwy_9jqSr/view?usp=sharing

By Tanaka Mrewa, CITE

CWGH Executive Director, Itai Rusike
Local health experts say Zimbabwe must strengthen and properly govern health taxes if it is to protect its fragile health system, following new recommendations by the World Health Organisation (WHO) to significantly raise taxes on sugary drinks and other health-harming products.
Zimbabwe’s health sector remains heavily dependent on donor funding, which has been steadily declining, raising concerns about the country’s ability to sustainably finance essential health services.
Earlier this month, the WHO urged governments to increase taxes on sugary drinks, tobacco and other unhealthy products, warning that weak tax systems are keeping harmful products cheap while fuelling obesity, diabetes, heart disease, cancers and other non-communicable diseases (NCDs).
The UN health agency said well-designed excise taxes can reduce harmful consumption while generating much-needed revenue for health systems under growing financial pressure.
“Health taxes are a cost-effective but still underutilised tool that can save lives, reduce disease and mobilise much-needed domestic resources for health,” Community Working Group on Health (CWGH) executive director Itai Rusike told CITE.
“At a time when official development assistance is declining, countries like Zimbabwe have very few options left if they want to sustainably finance their health systems,” he added.
Rusike said several countries had already demonstrated that earmarked health taxes can deliver both public health and economic benefits.
“South Africa introduced an excise tax on sugary drinks in 2018 and reported a significant reduction in purchases of taxed beverages. Botswana followed with a sugar tax in 2021, while Ghana increased tobacco taxes in 2023 and earmarked part of the revenue for health,” he said.
Zimbabwe has also taken steps towards domestic health financing through mechanisms such as the AIDS Levy, the Health Levy and, more recently, the Sugar Tax.
The sugar tax, officially known as the Special Surtax on Sugar Content, was introduced in 2024 and targets sugar-sweetened beverages to fund cancer diagnosis and treatment.
Initially set at US$0.002 per gramme of sugar, the tax was reduced to US$0.001 in February 2024 following objections from the beverage industry.
While welcoming the policy intent, Rusike raised concerns about governance and transparency in the use of the revenue.
“The sugar tax is collected by ZIMRA and deposited into the Consolidated Revenue Fund. That creates a real risk that the money can be diverted to other government expenses instead of cancer services,” he said.
“To protect public trust, there must be enabling legislation to ring-fence these funds so that every dollar goes where it was promised.”
He added that stakeholders were increasingly questioning whether money raised through the sugar tax was being used efficiently and whether communities were seeing tangible improvements in hospitals and clinics.
The tax has also had ripple effects along the sugar value chain, with beverage manufacturers and sugar producers reporting declining volumes and revenues.
However, Rusike said the broader public health context should not be overlooked, arguing that the long-term benefits of reduced disease burden and stronger domestic health financing outweighed short-term economic adjustments.
CWGH Executive Director, Itai Rusike
By 263Chat – Staff Reporter
The Community Working Group on Health (CWGH) says the country’s public health system is buckling under years of chronic underfunding leaving millions of citizens without adequate medical care.
In an interview with 263chat, CWGH executive director Itai Rusike said public health spending accounts for only a small fraction of total government expenditure leaving infrastructure and services unable to meet the population’s needs.
“Public health infrastructure is grossly inadequate to cater for the health-care demands of the citizens,” Rusike said.
He added that most health facilities, particularly in rural areas lack essential equipment, ambulances, medicines and supplies severely affecting the ability of health workers to diagnose, treat and manage medical conditions.
“Theatres and laboratories are usually not functional or do not have the staff to carry out tests. As a result, people are forced to turn to private sector services at catastrophic costs,” Rusike said.
The CWGH chief warned that the failure to retain qualified health workers has created serious gaps in service delivery with many patients suffering from poor service, negligence and misdiagnoses.
He also highlighted the hardships faced by rural patients many of whom must travel long distances to access primary health care while clinics struggle with basic water and electricity shortages.
“This situation underscores the urgent need for investment in Zimbabwe’s health sector to ensure that all citizens, especially those in rural communities, can access safe, reliable and affordable medical care,” Rusike said.
Meanwhile, the government has announced a major health infrastructure investment aimed at easing pressure on overcrowded referral hospitals and improving access to medical services.
Under the 2026 Zimbabwe Infrastructure Development Programme, ZIG$3.9 billion – equivalent to about US$140 million – has been allocated for the construction, rehabilitation and modernisation of health facilities nationwide.
Authorities say the programme will also fund medical equipment, ambulances, digital health systems and staff housing, measures intended to improve efficiency and retain health professionals.
The government believes the initiative will significantly improve healthcare access, particularly for rural communities that currently travel long distances to receive specialist treatment. -263Chat
263Chat is a Zimbabwean media organisation focused on encouraging & participating in progressive national dialogue

Click link for details:
https://drive.google.com/file/d/1NqzTA5TUmC0yG-WHN2pEXFChZj5zWXY0/view?usp=sharing


Robin Muchetu, Health and Gender Editor
THE High Court’s landmark ruling that struck down key parts of Zimbabwe’s restrictive abortion law as unconstitutional has drawn strong reactions from public health advocates and gender-rights organisations, who say the decision marks a long-overdue step towards protecting vulnerable women.
Justice Sylvia Chirawu-Mugomba ruled that Section 4(a) of the Termination of Pregnancy Act (Topa) of 1977, as well as the definition of “unlawful intercourse” under Section 2(1), are unconstitutional and invalid.
Parliament now has 18 months to amend Topa to align it with the Constitution and to incorporate protections required under the Mental Health Act.
Justice Chirawu-Mugomba decision followed an application by the Community Working Group on Health (CWGH) and Member of Parliament Nyasha Batitsa, who argued that the law unfairly excluded women with mental illness from accessing legal termination, even in cases of sexual exploitation.
The judge found that the decades-old Act fails to recognise that women with mental health conditions may be unable to consent to sexual activity and are therefore at heightened risk of abuse. By excluding them, the judge ruled, the law violates constitutional guarantees of equality, dignity, humane treatment and bodily autonomy.
“The statutory omission creates a discriminatory regime, forcing women to carry pregnancies that cause grave mental-health consequences,” Justice Chirawu-Mugomba said.
Although the affected provisions have been declared invalid, the order has been suspended for 18 months while Parliament amends the law. The ruling has also been referred to the Constitutional Court for confirmation.
Justice Sylvia Chirawu-Mugomba suspended for 18 months from the date of the order to enable the respondents to amend the provisions in the Termination of Pregnancy Act as cited to include mental health and conduct proscribed in Section 106 of the Mental Health Act.
“The above declarations of constitutional invalidity are suspended until such time as the Constitutional Court has confirmed the same in terms of section 167(3) of the Constitution of Zimbabwe. The above order of constitutional invalidity is referred to the Constitutional Court for confirmation in terms of section 175 (1) of the Constitution. There shall be no order as to costs,” she ruled.
CWGH executive director Mr Itai Rusike said the judgment marks a reflective shift in the country’s reproductive-rights landscape.
“It shifts the legal framework from a narrow, biomedical model of abortion, centred solely on physical survival, to a constitutional model grounded in dignity, equality and holistic health,” he said.
“Recognition of mental-health risk as a standalone indication for lawful termination modernises an area of law historically shaped through punitive colonial codes that disregarded women’s lived realities.”
Mr Rusike noted that the ruling elevates mental health within the country’s constitutional right to health and may have wider implications for health-sector reforms.
“This opens space to challenge insurance exclusions on psychiatric services, the chronic underfunding of mental-health care, and policies that treat mental health as secondary,” he said.
Mr Rusike said the decision also aligns Zimbabwe with regional and international obligations under instruments such as the Maputo Protocol and Cedaw.
Women’s rights groups said the court’s recognition of the vulnerability of institutionalised or mentally ill women, particularly under Section 106 of the Mental Health Act, is a major advance.
They argued that previous legal provisions offered little protection to women who cannot consent to sex yet were denied legal termination if they fell pregnant through abuse or exploitation.
Women’s Action Group (WAG) programmes officer Ms Vimbai Nyika said the ruling places new responsibility on the media to ensure accurate, sensitive coverage of abortion and sexual and reproductive health rights (SRHR).
“We want to strengthen the capacity of journalists to report ethically and sensitively on safe abortion and SRHR. With unsafe abortions happening around us, media narratives matter,” she said.
“They influence public understanding, policy debates and ultimately national productivity. The media has the power to educate, inform and support rights-based approaches to these issues.”
Zimbabwe’s current abortion law, passed in 1977 during the Rhodesian era, allows termination only when a woman’s life or physical health is in danger, when the foetus faces severe disability or when the pregnancy results from “unlawful intercourse”. Mental-health grounds are not recognised.
Applicants in the case argued that this omission violates constitutional rights to dignity and health, noting that mentally ill women cannot consent to sex and therefore must have access to legal termination.
—@NyembeziMu
… Ruling significantly expands access to legal abortion for mentally ill women and victims of institutional sexual abuse
By Staff Reporter, 17 November 2025

Human rights lawyer Tendai Biti argued for women with mental health challenges to be granted the right for legal abortion
By Staff Reporter, 17 November 2025
HARARE — The High Court has delivered a landmark ruling declaring parts of Zimbabwe’s abortion law unconstitutional, finding that provisions of the Termination of Pregnancy Act violate several fundamental rights, particularly the rights of mentally ill women and victims of sexual abuse in mental health institutions.
Justice Slyvia Chirawu-Mugomba, handing down judgment, ruled that section 4(a) of the law governing the circumstances under which a pregnancy may be lawfully terminated “to the extent that it excludes mental health” fails to meet constitutional standards and unjustifiably limits key rights such as dignity, equality, and the right to health.
The applicants, the Community Working Group on Health and Member of Parliament Nyasha Batisa, challenged the constitutionality of the law, arguing that it discriminates against mentally ill women by permitting pregnancy termination only under narrow physical-health exceptions.
They sought declarations that both s 4(a) and the definition of “unlawful intercourse” in s 2(1) of the Act are unconstitutional.
In a detailed 25-page ruling, Justice Chirawu-Mugomba found that the law’s failure to recognise mental health as a basis for accessing safe and lawful abortion imposes a discriminatory and unconstitutional burden on women with mental health challenges.
The judge noted that the applicants had “well-articulated the impact of the exclusion of mental health as a ground to access safe abortion,” concluding: “Therefore, s 4(a) in my view, to the extent that it excludes mental health, does not meet the standards enunciated in the constitution…
“It is clear that women with mental health challenges are treated differently when it comes to the permissible health-related grounds for termination.”
Justice Chirawu-Mugomba rejected the argument by the minister of health that mental health risks were already implicitly covered under “life-threatening” physical conditions, holding that such an interpretation would be “not explicit” and left vulnerable women without clear legal protection.
She emphasised that mental health is integral to overall health, citing evidence of “genuine challenges women experience with mental health, including those that may arise after childbirth.”
The judge also held that the definition of “unlawful intercourse” in s 2(1) is unconstitutional because it fails to include sexual abuse defined under s 106 of the Mental Health Act, which criminalises sexual intercourse with mental health patients.
The judge said in the November 11 ruling: “Excluding mental health in the definition of unlawful intercourse, as proscribed in s 106… denies women in such circumstances access to safe abortion services.”
She found that the omission violates multiple constitutional rights, including the right to life (s 48), dignity (s 51), equality (s 56), and reproductive health (s 76), noting that mentally ill women “face legal and procedural barriers to accessing necessary reproductive healthcare.”
The judgment sharply criticised the inconsistency between the Termination of Pregnancy Act and the Mental Health Act, observing: “The inconsistency between these legislative frameworks undermines the principle of equality before the law.”
While acknowledging parliament’s primary role in law-making, the judge said that courts are constitutionally required to intervene where rights are unjustifiably limited.
She noted: “Judicial intervention is necessary to uphold constitutional rights, fill legal gaps, or develop the law in line with evolving social values.”
The court considered whether to “read in” new provisions – a remedy used where a statute is unconstitutional due to an omission – but concluded that the applicants had not framed their requested relief with sufficient precision.
The judge ultimately declared portions of s 4(a) and s 2(1) unconstitutional but suspended the declarations, as required by section 175 of the constitution, pending confirmation by the Constitutional Court.
The judge ordered: “The above declarations of constitutional invalidity are suspended until such time as the Constitutional Court has confirmed the same… The above order… is referred to the Constitutional Court for confirmation.”
No order as to costs was made.
Rights lawyer Tendai Biti brought the application on behalf of Batitsa and the Community Working Group on Health. – ZimLive
By Gamuchirai Nyamuziwa | Oct. 31, 2025

The deficit is crippling the country’s ability to provide even the most fundamental services, the CWGH said.
ZIMBABWE’S public health system is facing a catastrophic shortage of nearly 58 000 skilled workers, a deficit so severe it requires the government to hire an average of 9 758 new staff annually until 2030 just to achieve basic health coverage, a new health sector position paper claimed this week.
The report by the Community Working Group on Health (CWGH), which lays out critical priorities for the 2026 National Health Budget, warned the current health worker establishment is out of line with the nation’s growing population and escalating disease burden.
The deficit is crippling the country’s ability to provide even the most fundamental services, the CWGH said.
It claimed as of 2023, Zimbabwe’s health workforce stock stood at just 47,5% of the national need, representing a “need based shortage of 57 543 health workers”.
This chasm between the required and actual staff levels has extensive implications on health outcomes, pushing the system to the brink of collapse, analysts also warned.
The report underscored the urgency for a resilient and motivated health workforce, a goal that remains elusive under current conditions.
“Therefore, it is essential to ensure availability of a resilient, motivated, and fit-for purpose health workforce,” the paper asserted, directly linking the staffing crisis to Zimbabwe’s inability to deliver on its universal health commitments.
To bridge this gap, the CWGH is making an unprecedented call for massive and immediate budgetary action.
“The government needs to demonstrate its commitment to expand MoHCC (Ministry of Health and Child Care) staff establishment by an average of 9 758 workers per year up to 2030 to meet the projected Health workforce need-based shortage,” the report stated.
This level of recruitment is deemed necessary to achieve 80% Universal Health Coverage and 99,1% disease burden coverage, targets that are foundational for the nation’s aspiration to become an Upper Middle-Income society by 2030.
The paper said termination of contracts for USAid-supported health workers had exacerbated the crisis, leaving critical gaps in health facilities and negatively impacting the quality of services.
The CWGH argued that the 2026 budget must not only fund new positions, but also absorb key roles previously supported by donor funds onto the government payroll to ensure sustainability and protect primary healthcare services for the most vulnerable. – Zimbabwe Independent.